|
Working with Babies: A Specific 4 Point Sequence for the Practitioner Toolkit Kate White, MA, BCBMT, RCST®, CEIM, SEP There are several common themes in my treatment room when working with babies. One is that a family calls me in the weeks after birth to say that their baby is not breastfeeding well. Working with babies is becoming more and more important, as we are seeing increases in tongue tie surgery, difficulty feeding, and birth trauma. The following is a description of my work for the enthusiastic learner of a mom and baby who came to solve feeding difficulties. Working with Babies Carrie* brought her baby to me because she was not breastfeeding comfortably. Her baby was 4 months old by then, and while she was gaining weight okay, she clicked and clamped down at the breast, making feeding painful for Carrie and uncomfortable for her baby, Alice. Whenever I meet a mother and baby for the first time, I am witnessing, watching, and feeling into the energetics of the relationship. I watch how she or he interacts with me, how they look at me, how they are in their bodies. John Chitty, RPP, RCST®, co-owner of the Colorado School for Energy Studies taught me to always recognize the baby as a spiritual being. He had a silent greeting for the baby:
For the Practitioners: Questions to ask mothers, initial session:
Then:
Repeat the mantra on the inside:
Then begin your palpation assessment. How is inhalation, exhalation (CST) How is baby holding her body What is baby saying with her hands? Feel with your hands, what is tight, what has ease? How is her skin color? Talk with the baby while you are doing all this, let her know what you are doing, even if she is breastfeeding or sleeping. How is the mother? Is she majorly stressed? If baby is not sleeping well, ask about her sleep. Anything else she wants to report. How are moods? Everything okay? Finally: What is right with your baby? What is going well?  Upon entry, I immediately saw Alice’s intrauterine constraint. She had been posterior and “asynclitic” meaning positioned “at an angle” in the maternal pelvis during the third trimester in utero. We discerned that she had been stuck since week 22 of pregnancy and grew her body in an extreme c-curve. Her placenta was anterior in the womb, and we guessed she had “gotten stuck” behind it somehow. Her sleep and other lying positions revealed a common pattern we call “fixed retroflection,”[1] or patterns of fascial tightening that compromise a baby so that there is difficulty breathing, feeding or even lying still on a flat surface. Sleeping is also difficult, the chronic pain from the tightness causes chronic agitation as the baby seeks relief, and digestive problems because of the stress and discomfort. These patterns can create limited range of motion in the neck and jaw especially. With a few delicate put potent bodywork sessions of Pediatric Function Bowen™ work and Biodynamic craniosacral therapy I was able to restore Alice’s body to function, but there was still much to do. Over a period of several months I completely released the extreme pattern in her body. [1] This is a term from Pediatric Functional Bowen™ work, a manual therapy developed by Judy Terwilliger. For more information see knowmor.org 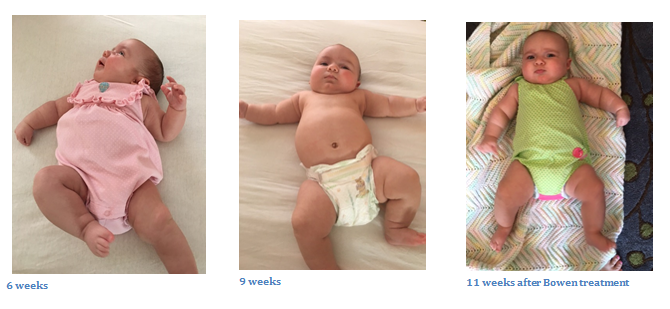 Pediatric Functional Bodywork™, parent education about the baby’s experience, infant massage instruction and movement, and Biodynamic craniosacral therapy are an excellent skill combination to help families with feeding, sleeping and general difficulty to soothe with their babies. Whenever I see a baby, there is a hold sequence that I most always perform because of their relationship to feeding and comfort. The first part of treating families with babies is the intake process, getting the birth story, and explaining the baby’s experience. Many parents also have trauma from birth or not being able to settle their baby. I name and normalize difficulty, and present a treatment plan. I talk with the baby, too, tell them everything I do and take in their communication with me, verbal and nonverbal.
The treatments often include a 4 point sequence: sacrum, occiput, temporal, and ethmoid/vomer. Sacral hold: Holding the sacrum always me to enter into touch relationship with the baby without too much alarm, plus discernment of the fascial pattern that might be at play. I can often release the sacroiliac joint here and allow fascial unwinding and facilitated movement[1]. Tightness in the hips can also impede jaw and mouth function, so releasing tension here helps babies suck, swallow, and breathe. Babies often down-regulate their autonomic nervous system with cranial touch to their sacrum. Parents see their baby relax, and they too, begin to relax and settle. You can see it visibly and feel it in the relational field. Occiput: Decompressing the cranial base is a must for most babies presenting with feeding difficulties, and is a go-to hold for almost any presenting pediatric issue. Compression during third trimester and during birth will decrease function of cranial nerves needed for breastfeeding, and jaw movements. For babies like Alice, the viscero-cranium is often adhered to the occipital base. Releasing the compression, creating space in the back of the baby’s cranium allows more function in tongue and jaw movements, suck, swallow and breathe function and range of motion to make head turns and expression for social engagement. Many babies have headaches from neck and head compression, too. Simple touch and massage techniques around the head and shoulders provide great relief and can be taught to parents. Temporal bones: Practitioners need to check the function of temporal bones as they have the jugular foreman, the aqueduct for cranial nerves IX, X, and XI, all of which play a major role in feeding and autonomic nervous system function. Optimal vagus nerve (cranial nerve X) function in the first 1000 days of life is key to human development. It is a lifeline to healthy function of many of the baby’s systems, especially the relational field with parents, feeding, digesting and the felt sense of safety. It needs to myelinate over the first six months of in relationship with the caregiver. If it is compromised in any way, it will affect the bonding and attachment that is survival for babies, and key to mothering and caregiving in early parenting. Often one side will be more affected than the other because of the lie side third trimester and subsequent compression during labor. In addition, fast births will often affect temporal bones by causing them to “freeze.” I often find the craniums of fast birth babies to be very affected by the rapidity of the birth. Moderate birth pacing and tempo allow for the baby’s head and body to respond adequately to the process. Fast births may put tissue (bones included) into a form a “shock” for lack of a better word. The vault hold, Becker’s hold, and then specific temporal holds allow the practitioner to check the motility of this bone, release and create space if there is compression, and encourage optimal functioning. Vomer/Ethmoid, or Ringing the Ethmoid Bell: Working on the midface completes the 4 point sequence when working with babies. First step is to assess the baby’s face. In general, you are assessing the baby’s body for fascial pattern and movement function. In the words of Pediatric Craniosacral and Lactation Therapist, Alison Hazelbaker, “Our babies should be relaxed!” The ones who come to see me are not. In the midface, follow the Law of Thirds[2]: The forehead, eye band, and maxillae/mandible should be equal to each other. I look for what I call the “squish factor;” The viscero-cranium is smashed into the neurocranium. I employ cranial touch into the midline bones of the face and encourage the rocking motion that the vomer and ethmoid have in relationship to the sphenoid and occiput. Sometimes, I will even encourage the viscero-cranium with a lift that is more advanced and often done when the baby is asleep, so it is harder to achieve in the office. This is a basic 4 point sequence that is part of my cranial evaluation of babies. I use many other points or holds when helping babies. I also support the mother, partner/father, and the baby further with working with the story of what happened, employing a trauma resolution approach combining practitioner skills of presence, pacing, naming, bodywork and verbal skills. I further employ storytelling and pacing to help repattern the story, plus facilitated movement and supported attachment to help the baby show their story and parents to listen. A Few Final Words After several months of careful work, baby Alice and her mother were deeply bonded and moved into the next phase of their relationship when Carrie returned to work. Carrie delayed her return until her baby could feed, sleep and move with ease, and she felt their relationship was established and free from the trauma of their experience. There were other difficulties in the relationship at the start. Alice has a tongue tie that was revised three times. The lack of fascial glide in the baby’s body prevented the tongue and jaw from movement that would have allowed better healing from tongue surgery. She had already had two of the surgeries before seeing me. We worked hard with the third revision, with bodywork before and after to free the tongue, and really, Alice’s whole body; babies use their whole body to breastfeed. Carrie also had PTSD from early childhood trauma, and the chaos of the difficulty with her baby reminded her of the helplessness she felt as a child. However, once we restored the breastfeeding relationship, the depression Carrie was feeling lifted. Breastfeeding trauma related to early feeding difficulties has risen significantly in the last few years from the increase in tongue tie diagnoses. Practitioners who wish to work with babies would benefit from specific classes on working with babies, lactation training, understanding tongue tie, and trauma resolution skills. A specific online class that where I presented Alice and her mother as a case study, plus the 4 point sequence presented here, working with tongue tied babies, and my holistic approach to working with families is found in my online classroom: https://prenatal-and-perinatal-healing-online-learning.teachable.com. Select Bristol Class. Coupon code for BCST/NA is: BCSTBABY for $30 off. Additional Resources: Bowen work: See John Wilks, https://www.therapy-training.com/book-shop Pediatric Functional Bowen™: See the work of Judy Terwilliger at knowmor.org See this video interview with her: https://vimeo.com/298012177 Working with Babies: A Five Point Therapy Method for Infants and Their Families by John Chitty Craniosacral Therapy for Children: Treatments for Expecting Mothers, Babies, and Children by Daniel Agustoni Video Sequences: Cranial Bones in Motion: https://youtu.be/tfKG9J9DiCw Sacrum: https://www.youtube.com/watch?v=RsI0n5Nwe-Y&t=5s Temporals: https://www.youtube.com/watch?v=hqQL-xmIcls Ethmoid: https://www.youtube.com/watch?v=MFF6SYvfLw0 [1] Facilitated movement is a term coined by Ray Castellino and Mary Jackson in their work with families and babies that allow babies to show their story of their prenatal time, birth and neonatal experiences. Showing story and having practitioner and parents “get” the story is an intervention in itself and can settle the issues of difficulty settling and sleeping. [2] I learned this from Jonathan Evens, DO who has an excellent online class for working with babies that anyone can purchase. See Kindredbe.com
3 Comments
4/10/2023 11:09:22 am
Brain trauma sounds serious. My wife hit her head the other day and is acting weird. She should probably get her brain scanned. 12/4/2023 03:38:07 pm
https://turkeymedicals.com/doctor Leave a Reply. |
AuthorKate White, MA, BCBMT , RCST®, CEIM, SEP lives in Charlottesville, VA ArchivesCategories |
 RSS Feed
RSS Feed